Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Abdominal Pain Assessment
Category: Medical
Topic: Abdominal Pain
Level: EMT
Next Unit: Organs of the Abdominopelvic Cavity
39 minute read
The Peritoneum--The Cloud that Rains on Everyone
The entire abdomen is covered by a shell of very thin tissue called the peritoneum. Not only does it form the roof, sides, and floor of the abdominal cavity (the "peritoneal" cavity), but it also turns at each of the abdominal organs--over, under, and around--to cover them. Some organs lie under it ("retroperitoneal"), such as the kidneys, ureters, bladder, blood vessels (including the aorta and inferior vena cava), and lymphatics; others are wrapped with it, anteriorly and posteriorly, as with the stomach and intestines and the female internal reproductive organs.
The peritoneum is unusual tissue in that the only pain nerves in it are those that fire off with distension. Therefore, abdominal/pelvic organ swelling from inflammation (infection) or bleeding will cause peritoneal pain. Unfortunately, since the peritoneum covers all of the organs, pain originating in one organ may be accompanied by a phantom sensation of pain from another organ, confusing the picture. Inflammatory fluids from a diseased organ, free-floating in the abdomen, may inflame other organs they come into contact with.
Abdominal Wall Pain and Carnett's Sign
Abdominal wall pain is the most overlooked source of abdominal pain, since
- overlying muscles can run horizontally and vertically, covering the entire abdomen;
- muscular injury and inflammation can be very painful; and
- the area over which torn, inflamed, strained, or ruptured muscle lies can fool one into thinking it's a condition of an abdominal organ beneath it.
The Carnett's test can identify whether pain in the abdomen is arising from an overlying muscle (the abdominal wall) or an underlying abdominal organ (in the peritoneal cavity).
When abdominal pain is related to posture (i.e., lying, sitting, standing), the abdominal wall should be suspected as the source of pain.
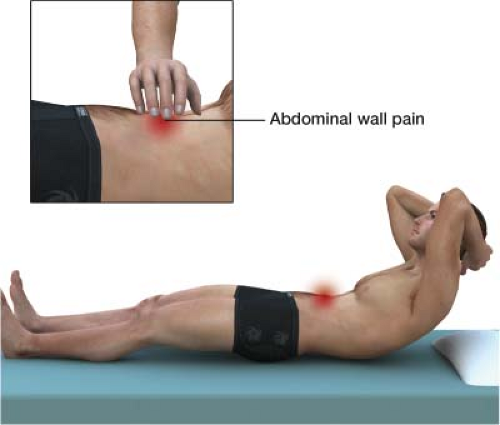
For the Carnett's test, simply lay the person supine and ask them to flex their neck (chin-chest) or straight-raise their legs. This will stiffen the abdominal musculature, which splints away true abdominal organ pain.
- If tenderness to palpation is UNCHANGED OR INCREASED when abdominal muscles are tensed, this is a positive Carnett's sign, and the abdominal wall is the likely origin of pain.
- However, if the result is iffy, assume it's abdominal organ-related as a prudent precaution.
The Acute Abdomen
An acute abdomen is severe abdominal pain or discomfort requiring urgent and specific assessment and diagnosis. It can be--but need not be--sudden: it can progress insidiously from mild to severe over a few hours' time.
While a normal abdomen during inspection and palpation demonstrates as soft and non-tender in all four quadrants, the acute abdomen during inspection and palpation is associated with
- nausea, vomiting, or
- diarrhea (with further classification as “excessive”; special attention is given to the presence of blood in emesis or stool) or to
- pain in any specific area/quadrant with or without palpation, or
- signs of shock or
- fever.
Rebound Tenderness

Depressing a place in the abdomen and then suddenly letting go can help determine whether there is diffuse peritonitis or blood or pus rolling around in the abdomen. If, instead of depressing the abdominal wall, the releasing of pressure causes sudden pain, this is called rebound tenderness.
Its value is that it indicates peritonitis and mandates rapid transport for an ongoing, worsening crisis. Rebound tenderness can also mean that something is freely moving to and fro, such as infectious fluids (exudates, inflammatory transudates, and pus) or blood. It usually indicates a surgical emergency and always requires transport until a disposition is made according to diagnostic imaging and evaluation at the appropriate surgical facility.
Rebound tenderness in an area other than the original site of pressing can point one to the real problem area. For example, if pressing and releasing in the left lower quadrant causes sudden pain in the right lower quadrant, this could indicate appendicitis.
Guarding

Guarding is, for lack of a better description, any resistance to your meddling. It can be either
- VOLUNTARY guarding (patient grabbing your hand before you touch him or her) or
- INVOLUNTARY, rigidity which is indicative of early peritonitis.
Involuntary guarding--the more serious of the two--is muscular rigidity which can be unilateral from a focal inflammatory condition such as an abscess or diffuse in full-blown peritonitis.
While guarding itself is one of the cardinal signs of peritonitis, it may not prove very important in the field in some circumstances because it is common, especially in children and those with low pain tolerance, and the distinction between voluntary and involuntary guarding involves subtleties of observation that are very subjective and difficult to separate.
Referred Pain
Referred pain occurs when pain is felt in a location that is different from the actual source of the pain. This happens at the spinal level where incoming pain nerves (afferent) reach the dorsal root ganglia. These afferent nerves can trigger depolarizations of other afferent nerves landing in the same area, causing those particular innervated areas to send signals out as efferent signals. The brain doesn't differentiate between these signals and combines them into one effect that travels up the spinothalamic tracts, which are the main pain pathways, to the brain where the pain is perceived.
Referred pain can be confusing because it can mimic pain that is coming from a different part of the body. For example, pneumonia can cause pain in the left upper quadrant of the abdomen, which can be mistaken for a ruptured spleen. It's important to understand the concept of referred pain so that the source of the pain can be accurately identified and treated.
The Abdominal Quadrants
Keeping in mind the overlapping external confusion the internal peritoneum may cause, the simplest way to demonstrate what an EMS provider might encounter with abdominal pain is by presenting different presentations based on the four abdominal quadrants:
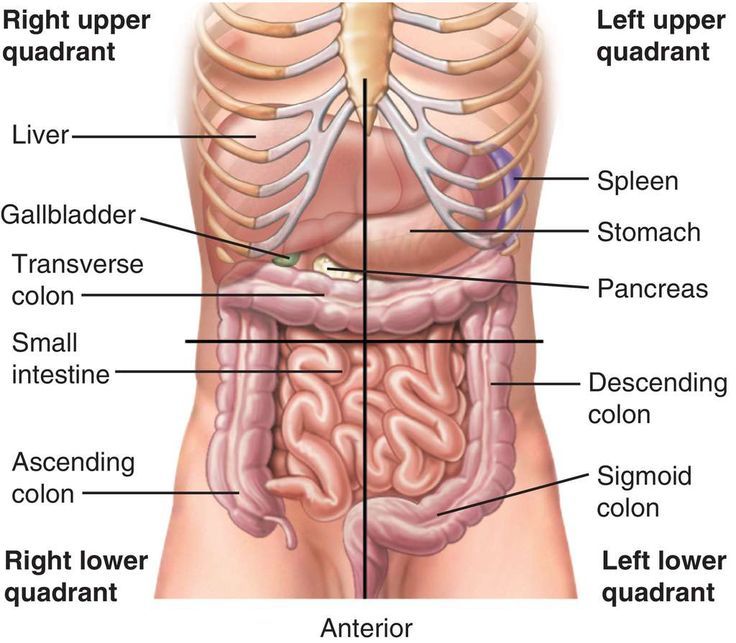
- RUQ: right upper quadrant, related to liver, gallbladder, ascending and transverse colon.
- RLQ: right lower quadrant, related to the lower small intestines, ascending colon, and appendix, and intestinal obstruction.
- LUQ: left upper quadrant, related to the stomach, spleen, transverse and descending colon.
- LLQ: left lower quadrant, related to the descending colon and rectum, and lower intestinal obstruction, constipation, and enteritis.
(These are each dealt with in the following units.)
Specific Acute Abdominal Conditions--the Famous Ones
Dissecting aortic aneurysm: cleavage of the wall of the abdominal aorta will give severe midline, shearing pain. A throbbing mass can be felt. More common in the elderly, it can be seen in anyone. This is a time-sensitive urgency because an ongoing dissection will quickly progress to rupture of the aorta and sudden death. (The aorta and vena cava are retroperitoneal structures, so leaking can cause back pain that doesn't fit neatly into any other symptom cluster.)
Gastrointestinal (GI) bleeding: GI bleeding can be caused by many different things including but not limited to
- ulcerative diseases,
- esophageal varices,
- hemorrhoids,
- anal fissures,
- liver diseases,
- infectious disorders,
- peritonitis,
- gastroenteritis,
- irritable bowel syndrome,
- inflammatory bowel disease,
- intestinal perforation,
- bowel obstruction,
- hernias,
- rectal foreign body obstruction,
- rectal abscess, and
- mesenteric ischemia resulting in necrotic (dead) bowel.
Upper GI bleeding: assessment findings and symptoms specific to upper GI bleeding include bloody vomit (color is red--fresh--or looks like coffee grounds--older, chronic).
Lower GI bleeding: Assessment findings and symptoms specific to lower GI bleeding include blood in stool (color is red--recent, or black and described as “tarry”--chronic).
Blood loss can be tolerated up to a point, especially with chronic GI bleeding. Acute GI bleeding, however, can quickly develop into shock with hypotension, tachycardia, and pale cool skin.
Appendicitis. This pain usually begins in the area of the umbilicus and migrates over 12-24 hours to the RLQ. Rupture is a life-threatening emergency and is accompanied by rebound tenderness in the RLQ, even if the palpation is in the LLQ.
Ruptured diverticulum--this is the same urgency as appendicitis, but it is usually due to diverticulosis, most commonly seen on the LLQ.
Intestinal obstruction. Blockage of the intestines can be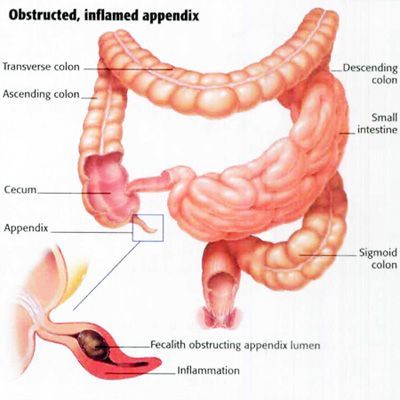
- anatomical, such as occurs in the kinks of internal scarring from previous surgery ("adhesions") or
- dynamic (physiologic), such as in narcotic interference of
- peristalsis ("ileus").
Blood or pus in the abdomen can also cause a dynamic ilieus. A quaint way to think about it is that the bowels are very cowardly organs: if ANYTHING in the abdomen is seriously wrong--internal bleeding, rupture, infection, obstruction, etc.--they shut down.
Therefore, the presence of reassuring intestinal findings, that is, if the patient is passing flatus and having normal bowel movements, these are good indications that nothing seriously wrong is happening.
But if there are worrisome findings, that is, diffuse abdominal pain, bloating, belching, or diarrhea, this predicts that all is NOT well and requires transport.
Cholecystitis: can cause any of the acute abdominal signs, but Murphy's Sign is specific for pain of gallbladder origin:
Palpate the area of the gallbladder under the liver edge and have the patient inspire deeply. This lowers the inflamed gallbladder against your fingers, which will almost always be painful with cholecystitis, although it can be painful with other acute abdominal conditions. (In other words, almost all cholecystitis patients will have a positive Murphy's sign, not all Murphy's signs are cholecystitis).
Renal or ureteral colic. A stone ("neprholithiasis") causes a severe, sudden, acute pain, usually unilaterally. It can be accompanied by a history of bloody urine.
Kidney infection ("pyelonephritis") can have the same symptoms but can be either unilateral or bilateral. The difference between a stone obstruction and an infection in the kidneys is that in pyelonephritis there is usually a high fever. A stone in the ureter will distend the ureter above it as it tries unsuccessfully to pass, with progressive dilation and pain above the obstruction (like "stepping on a garden hose.") Pain from a ureteral stone will be more toward the involved flank.
Management
General management for patients with acute or progressive abdominal pain includes
- verifying scene safety and donning personal protective equipment,
- verifying and supporting the ABCs: a patent airway, breathing (adequate respiration and ventilation), and assessing and managing for adequate circulation. Also,
- placing the patient in the position of comfort and providing emotional support are integral parts of the management.
NOTE: In pediatric patients, vomiting/diarrhea can quickly cause shock through vascular collapse seen in severe dehydration. In geriatric patients, abdominal pain may be related to heart attack. Geriatric patients may not exhibit rigidity or guarding during acute abdominal conditions.
Pediatric Abdominal Pain
There are many anatomic and physiologic differences in children that affect the pathophysiology associated with acute abdominal conditions.
Assessment should include a thorough history.
Physical findings found more frequently in children include
- dehydration caused by vomiting, which may represent possible appendicitis (common in children);
- abdominal pain from constipation, and
- vomiting associated with gastrointestinal (GI) bleeding.
Management should include focus on the ABCs (maintaining patent airway, breathing--adequate respiration, oxygenation, and ventilation, and circulatory support) as well as proper positioning and emotional support. The parents can be just as distraught as their child, so communication and information is very important to avoid additional drama and difficulties in management.
Postoperative Complications
Adults, children, and adolescents can have the same post-operative complications, which will all fall into one of three categories:
A.) Infection
B.) Bleeding
C.) Damage to other structures
Surgeries for appendicitis, kidney obstruction, intestinal conditions such as Crohn's and ulcerative colitis bring with them fear of post-op infection and bleeding (internal). These are transport-worth emergencies. Usually, post-op pain during recovery gets less each day, so anyone recently postop (< 7 days) should be transported if there is fever or when there is any discomfort that has gotten worse over 24 hours. This is especially true with the newer "minimally invasive surgery" and robotic surgery, where intra-op damage may be difficult to notice until suspected by post-operative complications.
Assessment
Besides a history, assessment techniques for acute abdomen include
A.) Obtaining the patient's chief complaint and its presentation (pain--sharp vs. dull, intermittent vs. constant, etc..")
B.) Inspection, and
C.) Palpation
Communication with patients who are experiencing an abdominal or gastrointestinal condition or emergency should be concise, clear, and easy to understand, often with yes or no questions, since requiring the patient to speak in more elaborate terms may increase pain or discomfort. Simple directions that do not require verbal responses are a good idea, such as, "Point with one finger exactly where the worst pain is," which is probably the single, most important question you can ask.
Remember to be supportive and patient. Documentation should always be thorough and concise, objective and professional, and detailed with correct terminology. Use the 4 quadrants as designated areas for documentation:
- RUQ
- LUQ
- LLQ
- RLQ
In documentation, positive findings are important, but so are the pertinent negatives and should be part of the documentation. For abdominal pain, pertinent negatives would include:
- "No rebound tenderness."
- "No nausea."
- "No bloating or swelling.
- "No diarrhea, constipation, or bloody stool."
Normal findings during inspection and palpation are a soft and non-tender abdomen in all four quadrants, with a history of recent normal bowel movements and passing flatus. Remember, there can't be anything terribly wrong if the bowels are working fine.
Abnormal findings during inspection and palpation are
- pain to palpation anywhere,
- any rebound tenderness,
- nausea, vomiting, or diarrhea (with further classification as “excessive;” and special attention is given to the presence of blood in vomitus (emesis--hematemesis) or stool).
Changes in bowel habits include constipation, diarrhea, dark and tarry stool, and mucus in the stool; changes in urination include pain with urination ("dysuria"), increased or decreased urinary frequency, and abnormal color and abnormal odor; weight loss, belching/flatulence, concurrent chest pain, pain to any specific area/quadrant with or without palpation, guarding, tenderness, distension, signs of shock, and fever are all noteworthy for documentation.
A note about urine color and odor: urine is typically an amber color, but dehydration can darken this considerably, almost to the point of looking like there is blood present, which can be misleading; also, urine smells like urea, but there is a difference between a strong odor (as in dehydration) and a foul odor (as in malodorous infection or pus).
Transport Decisions
In the field, transport decisions for patients who are experiencing an abdominal or gastrointestinal condition or emergency should be based on overall patient condition and provider experience. Consider ALS intercept in BLS units.
- Abdominal pain anywhere with rebound tenderness.
- Bloating with absent or hyperactive bowel sounds, such as "rushes." Normal bowel sounds are gurgling and not associated with bloating or pain.
- Blood in the vomit (hematemesis, as bright red or older, coffee ground-like).
- Same with blood in the stool.
- Mucus in the stool of recent origin. Patients with Crohn's and ulcerative colitis may live with stool mucus (and bleeding) as a chronic symptom, but new-onset mucus can indicate bowel death from mesenteric ischemia.
- Any abdominal pain associated with a fever.
- Any RLQ pain. The RLQ is so famous for appendicitis that you can't go wrong transporting anyone with it, even without nausea (although most appendicitis is accompanied by nausea).
- Any LUQ pain associated with recent trauma (car accident, fall on a blunt object, etc.) Like the RLQ and appendicitis, the LUQ and spleen rupture is a famous mandatory transport indications.