Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Surgical Cricothyrotomy Procedure
Category: Airway
Topic: Advanced Airway Management
Level: Paramedic
Next Unit: Continuous Positive Airway Pressure
13 minute read
Surgical Cricothyrotomy Procedure
A traditional cricothyrotomy is a true surgical procedure, it involves cutting through the layers of tissue that overly the base of the larynx in the neck, allowing for placement of an endotracheal tube below the larynx. It allows for rapid access to the lower airway when all other means of gaining a patent airway have failed and your patient will die if an intervention isn't rapidly accomplished.
While quick and easy to perform, it is considered a true surgical procedure, making cleanliness and attention to procedural detail imperative. This section will review the details surrounding the surgical method of cricothyrotomy, details surrounding the intervention of cricothyrotomy itself can be found in the section "percutaneous cricothyrotomy."
Indications, contraindications, complications, and limitations
INDICATIONS: Cricothyrotomy is a last-ditch effort to save a patient's life and should never be attempted if the patient's airway can be controlled by less invasive means (e.g., orotracheal or nasotracheal intubation). Surgical cricothyrotomy is the quickest and most effective method of obtaining a sub-laryngeal airway, as it may be needed in severe facial trauma, C-spine injury, anaphylaxis with complete obstruction, and inhalation injuries that cause massive edema.
CONTRAINDICATIONS: Insufficient training is the only contraindication for a surgical cricothyrotomy. Young age is a relative contraindication as the incision into the larynx can result in strictures later in life. For this reason, the needle method is preferred in children under 12.
COMPLICATIONS: The complications listed in the section "percutaneous cricothyrotomy" all apply to the surgical method. However, the surgical method is notable for having a higher risk of causing laryngeal abnormalities later in life if the patient is below 12 years old. For this reason, in young patients, the needle method is preferred. The surgical method also imparts a significant risk of fatal bleeding if done incorrectly due to the large blood vessels in the neck.
LIMITATIONS: As will all cricothyrotomies, obstructions beneath the level of the larynx base are not corrected with this procedure. Inhaled foreign objects have the potential to be lodged deep in the trachea and will still obstruct ventilation. All forms of intubation have limited utility if the patient's lungs are full of blood, pus, or other fluid.
Equipment Needed for Surgical Cricothyrotomy
Commercially prepared cricothyrotomy kits are available through a number of manufacturers. If a kit isn't available, the following equipment must be gathered:
- Sterile gloves and drape.
- Scalpel blade.
- Size 6 or 7 ET tube or tracheostomy tube (if ET tube is used, a Size 6 is preferred for an average adult).
- A syringe for inflating the ET tube balloon
- Antiseptic solution.
- Oxygen source.
- Suction device.
- Bag-valve-mask.
Suture, gauze, saline, and additional gloves should be close by in case of additional bleeding or unexpected complications.
Surgical Cricothyrotomy Procedure
- Position the patient to allow for unobstructed access to the anterior neck.
- Apply lidocaine (if indicated and protocols allow) and cleanse the site with an antiseptic solution such as betadine.
- Identify landmarks.
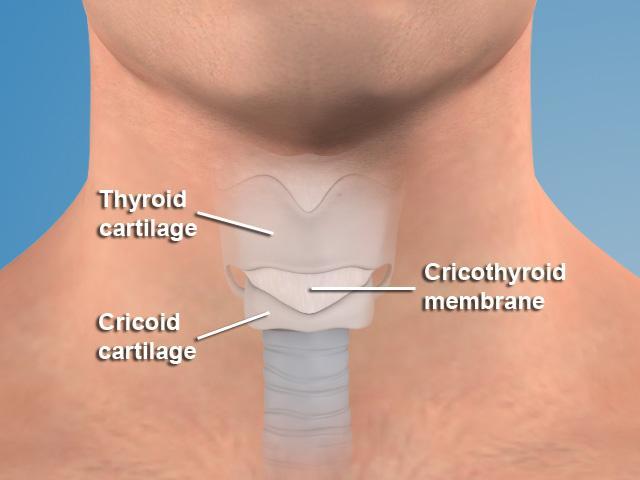
• Thyroid cartilage.
• Cricoid cartilage.
• The cricothyroid membrane between them. - Palpate the thyroid cartilage (the first prominent landmark on the anterior neck), the cricoid cartilage (a second bump inferior to the thyroid cartilage), and the area between them (this is the cricothyroid membrane).
- Using the non-dominant hand, stabilize the area by placing the thumb and middle finger on either side of the thyroid cartilage, allowing the index finger to palpate the membrane.
- With the dominant hand, make a midline vertical skin incision, approximately 3 cm long and skin deep over the cricothyroid membrane (this may result in minor bleeding, but avoids the major arteries--a good thing!).
- Palpate the cricothyroid membranes through the incision, using the non-dominant hand. With the dominant hand, make a horizontal incision through the membrane causing a pop sensation as the scalpel pierces the membrane and enters the trachea.
- Using a partner with the tracheal hook at the superior end of the incision, retract the skin upwards and then remove the scalpel.
- Dilate the horizontal membrane incision vertically with the Trousseau dilator using the non-dominant hand, then insert the tracheostomy tube between the two blades of the dilator, towards one side of the patient, then after entering the membrane, rotate it 90-degrees and advance it inferiorly.
--Dilating the incision vertically will meet more resistance (from the thyroid cartilage above and the cricoid cartilage below, than if you were to it horizontally, so be ready to spread the dilator against this vertical pressure from above and below. - Remove the obturator and insert the inner cannula; make sure to lock it in place.
- Inflate the balloon with manufacturer-set air pressure, and attach the tube to a BVM and ventilate.
CHEAT SHEET-- Incisions are: Vertical-Horizontal-Vertical
- Vertical on the skin to avoid lateral vascular structures.
- Horizontal on the cricothyroid membrane, and at a downward angle to avoid cutting the vocal cords.
- Vertical again (extension of incision via Trousseau dilator).
Post-intubation reassessment and management
Immediately following intubation carefully monitor every vital sign as countless complications are possible; heart rate, blood pressure, SPO2, ETCO2, and respiratory rate are all critical.
Following the immediate post-intubation period, use the mnemonic DOPE for factors that could affect your now intubated patient while they are in transit.
- D – Displacement/Dislodged tube.
- O – Obstruction or clamped tube.
- P – Placement in the R mainstem bronchus or esophagus.
- E –Equipment: the tube or other equipment may have malfunctioned requiring replacement.