Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
RLQ Abdominal Pain
Category: Medical
Topic: Abdominal Pain
Level: Paramedic
Next Unit: RUQ Abdominal Pain
27 minute read
The Major Players in the RLQ
The right lower quadrant (RLQ) of the abdomen contains the:
- Appendix.
- Right ureter.
- Small intestines, mainly the ileum.
- Ascending large colon, beginning at the cecum, where the appendix is.
- (in women) the right ovary and right fallopian tube (uterus is a midline organ).
Appendix
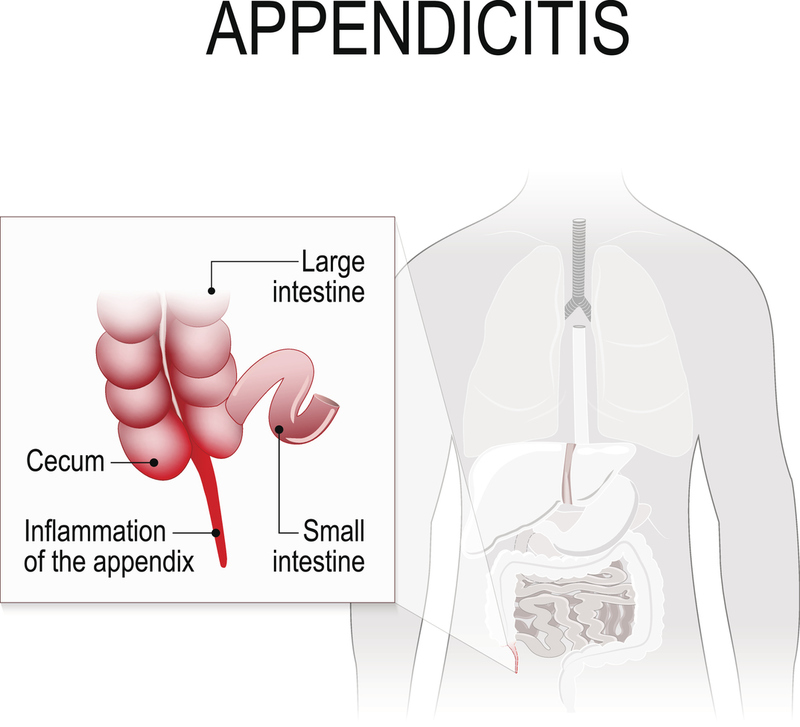
Often thought of as an evolutionary holdover, the appendix is an immunological organ, one of many (e.g., spleen, tonsils, etc.). It is a one-way street extending as a worm-like dead-end structure from the cecum (beginning of the ascending large colon). Its thinness and difficulty exit allows hardened pieces of feces (fecaliths) and dietary debris (seeds, corn husks, etc.) in the GI tract to get stuck in it, promoting infection. If abscess formation occurs, it can rupture pus and infectious material into the abdomen, causing generalized deadly peritonitis.
Of the causes of RLQ pain, the appendix is the most frequent flier when it comes to transport for abdominal pain. While the ureters are bilateral and small bowel symptoms can cross quadrants, the appendix is exclusively in the RLQ.
The typical course of appendicitis: because of a strange referred pain phenomenon, it
- begins as pain around the navel,
- and then over a day, the pain migrates to the RLQ (to an anatomical reference called "McBurney's Point"- a point on the abdominal wall that lies between the navel and the right anterior superior iliac spine) as a sharp pain frequently accompanied by dull pain in the rest of the RLQ. It is accompanied by a
- low-grade fever (99--100ºF/37.2-37.8ºC ) and with—almost always—
- nausea.
Lack of a fever does not rule it out. Although antibiotics might cool such an infection down, the removal of the appendix is to prevent rupture and to prevent recurrence, which is likely. Appendicitis is most common between the ages of 10 and 35 and affects about 5% of the population during their lifetimes and can occur at any age.
CAVEAT: The life-saving caveat has always been: RLQ pain is always appendicitis till proven otherwise.
Mild appendicitis that spontaneously resolves can leave behind baggage, i.e., adhesions (see below), but a rupture is a life-threatening emergency, spilling pus and infectious/fecal material into the peritoneal cavity. Therefore, all cases of appendicitis are treated as if they were already emergencies. The definitive treatment for appendicitis is surgical removal of the appendix, so your primary motivation should be rapid transport. Be prepared to address hypoperfusion (shock) en route.
Ureter
The paired ureters (one extending into the LLQ and one into the RLQ) drain collected urine from their respective kidneys and travel under the floor of the abdomen (retroperitoneal) to the pelvis where the drain is not the right word, because of each exhibit undulating musculature that “milks” the urine down the line (peristalsis) and spits urine into the bladder every few moments. Like all structures covered with the lining of the abdomen (peritoneum), which is very sensitive to distension, two presentations of emergencies involving the ureter will involve you:
- URETERAL SPASM: This can be caused by a urinary tract infection, but more typically is produced by a stone.
- OBSTRUCTION from a stuck stone trying to pass.
The pain from an obstruction or spasm of the ureter is
- colicky,
- sharp,
- severe, and
- intermittent (comes in waves).
It is usually limited to the respective flank (side of the abdomen). It is painful enough to cause collapse. Although not life-threatening, its presentation of pain is so dramatic you won't be confused about whether the ER is needed.
The pain originates on the one side (here, the right) and radiates downward, more dramatically when the stone is traveling. The urine is often blood-tinged, which you probably won't be assessing. As with any pain presenting on the right side, however, the appendix must be considered.
Large Bowel (Usually referred to as simply "the colon")
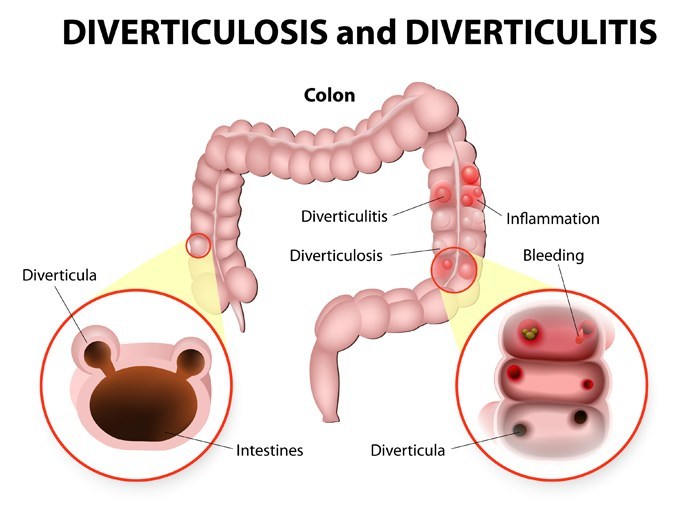
DIVERTICULOSIS/DIVERTICULITIS: a weakness in the bowel wall can cause a sac-like protrusion (diverticulum), which can get infected (diverticulitis) and create pain, usually from its very location. Although it is usually in the LLQ, it can occur in the RLQ occasionally. If hard fecal pieces (fecaliths) cause blockage, the diverticulum can rupture, just like an infected appendix. Usually, diverticulitis can be treated medically (antibiotics and diet), although 15% will require surgical removal of the diseased segment.
Small Bowel (Usually referred to as simply "the intestines")
The small bowel usually minds its own business (digesting and passing food onward toward the large bowel). However, infections of the abdomen, adhesions (see below), or cancer can cause obstructions, and the RLQ is no exception because the small intestines, all twenty feet, are primarily in the lower abdomen.
CROHN DISEASE: an inflammatory condition through the wall of the intestines that can lead to strictures and obstruction. Although it most frequently involves the ileum in the RLQ, it can happen elsewhere, so the abdominal pain is not limited to the RLQ. Suspected obstruction requires transport.
ADHESIONS: abnormal connections between tissues in the abdomen, which can make what are stuck together relatively immovable, leading to obstruction.
The abdomen is very vigilant to infection and inflammation, stimulating bowel fat to migrate toward such an area to wall it off from the rest of the body. The human body is no stranger to walling off infections, as is seen in abscesses. Internally, this protection, after healing, sticks areas together, sometimes creating a kink in the bowel that can make passage of bowel contents more difficult than when this area was free. This can distend the bowel to create a colicky, sharp pain. Such impediment to fecal movement is usually incomplete ("incomplete obstruction"), but when complete is called a "complete obstruction."
RLQ PAIN OF UNDETERMINED ORIGIN IN WOMEN: With the right ovary so close to the appendix, inflammation or infection of either can cause these two structures to “adhese” together, sometimes making a three-part adhered mass with bowel fat or peritoneum. This creates confusion when trying to differentiate between an ovarian process or appendicitis, which is a moot point, since this presentation--no matter what the cause--warrants transport. Even without any combined ovary appendix, i.e., no adhesions, both are in the RLQ and can evoke RLQ pain.
INTESTINAL OBSTRUCTION: usually fleeting in its painful presentation, adhesions (or the scarring seen in Crohn’s disease) can occasionally cause an obstruction that becomes a surgical emergency. Partial obstructions are treated with a liquid diet so as to not challenge the area. Adhesions are not exclusive to the RLQ, but can occur anywhere in the abdomen.
Abdominal Pain in Women
Abdominal pain in women is further detailed in "ABDOMINAL PAIN" in the section list, "ADOLESCENT AND PEDIATRIC GYNECOLOGY."
Because the female anatomy incorporates the reproductive elements for growing and delivering babies, it warrants special attention.
OVARIAN CYST: the ovary on the right is the counterpart to the one on the left. In a normal monthly cycle, a follicle ripens in preparation for the release of an egg (ovulation). If that follicle becomes exaggerated, growing to more than 2 centimeters, it is then deemed a cyst.
The pain from an ovarian cyst is
- sharp,
- one-sided, and
- specifically isolated enough such that a woman can point to it with one finger.
When it ruptures, the pinpoint pain suddenly stops, but this relief is soon replaced with a
- vague, spreading dull ache or burning sensation across the pelvis.
This represents the sudden release of the distension via cyst rupture, replaced with the pain from the leaking bloody fluid into the pelvis. It is not necessarily an emergency unless the amount of internal bleeding is enough to lead to signs and symptoms like an acute abdomen or tachycardia and hypotension (shock).
IN THE FIELD, you won't have to know the distinction between an expanding, leaking, or ruptured cyst, but will only have to act on RLQ pain or generalized abdominal pin, which in women warrants transport, especially for those of childbearing age.
ENDOMETRIOSIS: Another source of pain in the female pelvis/abdomen is the unfortunate implantation of menstrual-like tissue which can cause burning or aching pain on the side it resides (RLQ or LLQ). Since this is hormonally active tissue—just like the lining of the uterus—its flares are timed with the menstrual cycles, giving a crucial clue to the source of the pain and the diagnosis.
NOTE: Rarely, endometriosis may occur far from the pelvis--in the lungs, nose, or brain, giving misleading signals with nosebleeds, hemoptysis, or even strokes, respectively--all of which will also coincide with the monthly "period." Weird, but true--keep this in mind in the field, although you won't see this on the test.
FALLOPIAN TUBE: each fallopian tube can transport an unfertilized egg--or one that’s fertilized--from the ovary to spill into the uterus, which is midline in the pelvis. Two sources of fallopian tube pain are
- ectopic pregnancy, due to distention from a growing embryo/fetus; and
- salpingitis, due to infection, usually from sexually transmitted diseases such as gonorrhea and chlamydia.
Ectopic pregnancy is a life-threatening emergency, and salpingitis is a fertility-threatening emergency. They are both related because the most common cause of ectopic pregnancy is the internal tubular scarring from the salpingitis of STDs, which can hang up a migrating fertilized egg on its way to the uterus.
CAVEAT: This makes RLQ (or LLQ) pain from either STDs or ectopic--and you probably won't be able to call it--transport-indicated. Internal bleeding from a ruptured ectopic pregnancy can cause a life-threatening hemorrhage, so is a surgical emergency.
CAVEAT: A sudden collapse of an otherwise healthy woman or girl of childbearing age is to be considered shock from an ectopic-related internal hemorrhage till proven otherwise. (Transport, of course!)
PREGNANCY: lest we forget, pregnancy—with its expanding and rising central uterus—will shove the things that normally sit in the RLQ into the RUQ. One can only imagine the challenge that this would present when appendicitis—the most common cause of an acute abdomen in pregnancy—is confused with gallbladder or liver complications of pregnancy.