Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Pelvic Anatomy
Category: Trauma
Topic: Orthopedic Trauma
Level: AEMT
Next Unit: Pelvic Fracture Pathophysiology
14 minute read
Understanding the anatomy of the pelvic girdle is essential for assessing and understanding the underlying patterns of injury that define trauma to this region.
For the purposes of the national registry exam, understanding the positioning of major bones, muscles, and ligaments is key.
Only a basic understanding of the visceral organs in the area is necessary.
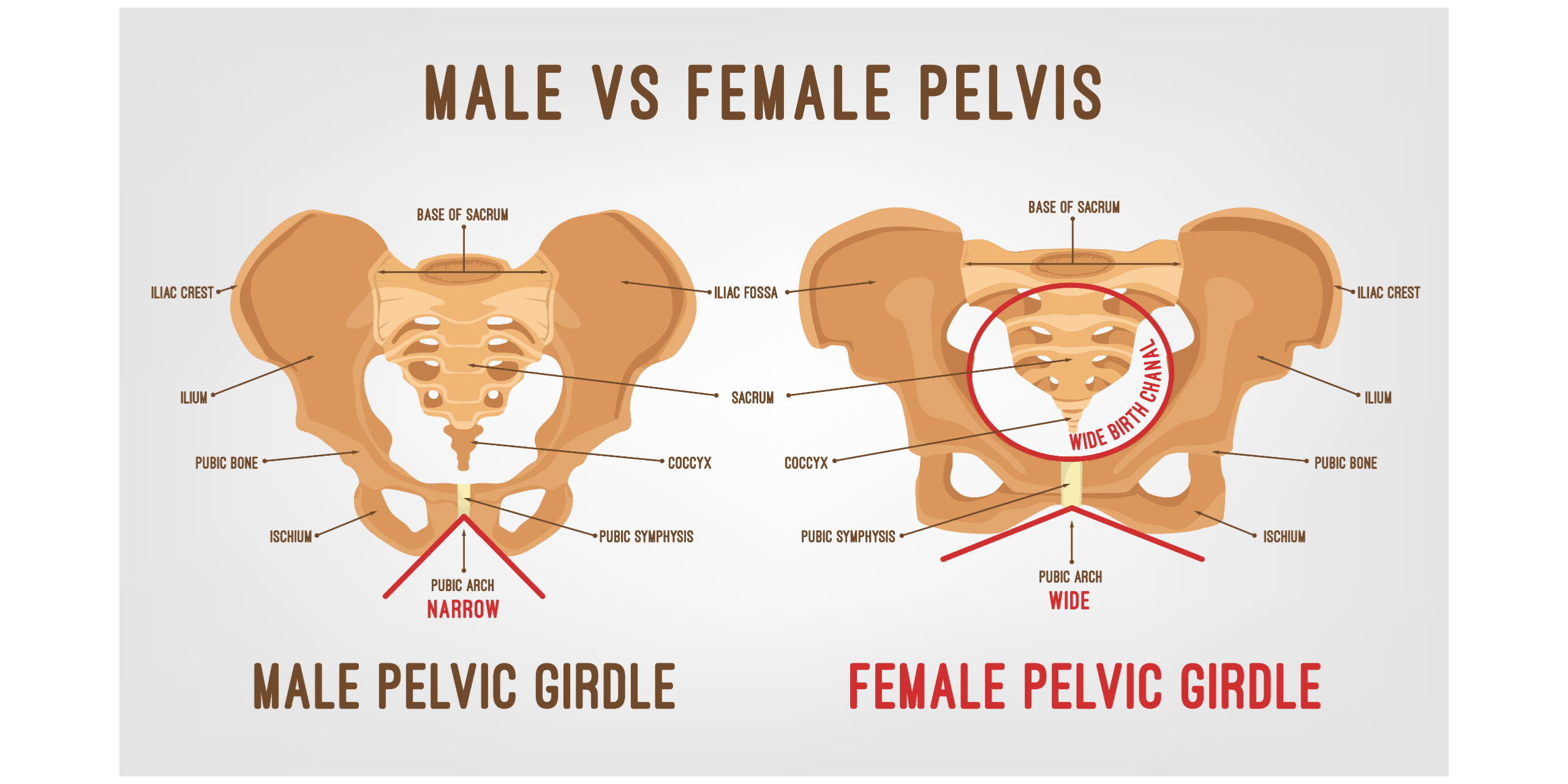
Bones
The girdle is made up of the fused sacral vertebra and two INNOMINATE (aka "hip") bones. The innominate bones are divided into several major anatomical areas which act as the attachment points for major muscles.
- SACRAL VERTEBRAE: These bones make up the very end of the spine. They protect the nerves that come from the base of the spinal cord and innervate the hips/legs. This area is also surrounded by a major plexus of veins.
- ILIUM: The largest component of the innominate bone, considered "the scapula of the pelvis," it is a large wing that is covered on both sides by muscle. When you place your hands "on your hips" you are putting them on this structure.
- ISCHIUM: A small cousin of the ilium, this structure makes up the "seat" that your body rests on when sitting in a chair. This structure forms a ring called the "obturator canal" by interacting with the pubis.
- PUBIS: This is the anterior and medial component of the pelvis, the bone you feel directly above the genitalia is the two pubic bones, the muscles that act here will bring the legs together "adduction."
Muscles
Knowing the exact muscles of the leg is not important, but knowing how they apply force to the pubic girdle is vital. A basic understanding will allow you to better appreciate the danger of ambulation and muscle spasm in the setting of injury.
- GLUTEAL muscles are located posteriorly and are closely associated with the ilium. Some put posterior and downward force on the ilium to pull the leg backward. Others act to help abduct the leg from the body by again putting downward and lateral force on the ilium.
- ANTERIOR THIGH muscles in this region pull downward on all parts of the pelvic girdle to raise the upper leg, bringing the knee towards the head.
- MEDIAL THIGH muscles act to bring the leg inwards ("adduct"). It does so by pulling on the pubis in a lateral direction.
- POSTERIOR THIGH muscles--some of the largest muscles--act to extend the leg in conjunction with the gluteal group, but they put downward and rearward force on the ischial ramus, as opposed to the ileum.
Ligaments and Symphysis
LIGAMENTS: There are two major groups of ligaments that provide nearly all the structure of the pelvis.
- The FEMORAL LIGAMENTS act to stabilize the ball and socket joint of the hip, connecting to the ilium and the ischium.
- The SACRAL LIGAMENTS are responsible for the major connection between the three bones of the pelvis. They form a web of connecting tissues that stabilize the pelvic ring.
PUBIC SYMPHYSIS: vital to the stability of the pelvis. It is a dense collection of tissue that bolts the pubic "anterior" section of the hip bones together.
Vessels, Nerves, and Viscera
VESSELS
ANTERIOR: The iliac and femoral vessels run anterior to the bones of the pelvis, making them most apt to injury in trauma to the tissue or bones of the anterior pelvis. The external iliac arteries branch into the femoral arteries and others, making the iliac vessels in harm's way higher up the iliac crest and the femoral vessels endangered below this. (The femoral artery branches from the external iliac artery about where the flexion of the leg is with the hip.)
Because the aorta is basically a midline structure (the vena cava also, but slightly to the right of midline), the more medial the pelvic trauma, the more likely hitting these; the more lateral, the less likely.
- The femoral arteries track anterior to the ilium and medial to the femur. These split from the aorta anterior to the sacrum.
- The Illiac vessels track through the large ring made by the pelvic bones, along the medial surface of the ileum.
POSTERIOR: The sacral venous plexus is one of the most commonly injured elements in the pelvis during any posterior fracture. The venous plexus is particularly vulnerable given its large size and close association with breakable bones. It is the site of significant bleeding since it is an "intersection" of numerous collateral venous flows from the other venous plexi (of the rectum, bladder, and genitourinary areas), all meeting in the sacroiliac and sacral areas.
NERVES
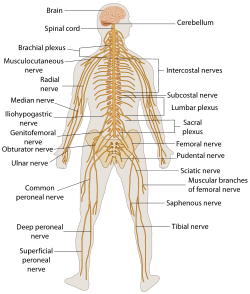
Major nerve pathways exist throughout the pelvis, both anterior, medial, and posterior to the ilium, with the sciatic nerve running just above the ischial ramus.
VISCERA
The major organs in the pelvic area are
- the bladder,
- intestines,
- rectum,
- ovaries,
- vagina,
- ureters, and
- prostate.
Each of these can be damaged by fractures of blunt trauma in this region. [This will be reviewed further in the PATHOPHYSIOLOGY OF PELVIC FRACTURE section]
NOTEWORTHY: Chest injuries, by far, have the strongest association with pelvic fracture. Injuries to the chest wall are extremely common in high energy mechanisms of injury. The bladder and Intestines lie within the pelvic cavity and are commonly injured, but not as often as the anterior chest!