Lighted Stylet and Fiber Optic Intubation
Category: Airway
Topic: Advanced Airway Management
Level: Paramedic
Next Unit: Percutaneous Cricothyrotomy
14 minute read
Lighted Stylet and Fiber Optic Intubation
Lighted stylet intubation is a variation of traditional, nasal, or digital intubation technique that gives the rescuer additional information while performing the procedure. It can be added to these other methods when intubating a difficult airway to increase the chances for success and lower the period of time the patient is apneic.
Indications, Contraindications, Complications, and Limitations
Many of the same indications, contraindications, and complications as traditional endotracheal intubation apply to Lighted stylet intubation, those factors are reviewed in detail in the section "Endotracheal intubation." The factors that differ are discussed here.
INDICATIONS: The use of a lighted stylet can be done preemptively if a difficult intubation is expected, or more commonly, following one or two failed intubation attempts. It can be used in any nasal or oral intubation.
CONTRAINDICATIONS: The only contraindication to adding the lighted stylet is severe obesity. Apnea is a contraindication for nasal intubation.
COMPLICATIONS: the complications of lighted stylet use are identical to any blind ET tube insertion technique, a chance of intubating the esophagus, potential trauma to the larynx, and the standard complications that follow the use of any ET tube.
LIMITATIONS: The limits of the lighted stylet are evident in bright environments as this technique relies on the light shining through the skin.
Procedures
- Pre-oxygenate the patient
- Assemble the equipment required for your desired method of intubation plus the lighted stylet (make sure the light is white, tight, and bright!).
- Check your tube cuff for proper ability to inflate, lubricate the tube, and insert the stylet into the tube until the bulb lies just distal to the tip of the tube, not extending past the end.
 Remember to bend the stylet over the proximal end of the tube so that it doesn’t move, and bend the whole combined unit into a loose “J” shape.
Remember to bend the stylet over the proximal end of the tube so that it doesn’t move, and bend the whole combined unit into a loose “J” shape.- Stand at the head of the patient (R of L side approach is acceptable if this is not possible), open the patient’s airway or remove the present adjunct, grasp the tongue with gauze and pull it forward.
- Turn on the light on the stylet and insert the lubricated tube into the mouth.
- Advance smoothly over the back of the tongue, into the hypopharynx and then into the laryngopharynx.
- Do not force the tube. If resistance is met, the provider should roll the tube between the fingers causing the distal tip to gently move from side to side, while continuing to advance the tube.
 A transilluminating glow through the anterior neck indicates where the tip of the tube is.
A transilluminating glow through the anterior neck indicates where the tip of the tube is.
- If the light is difficult to see, consider dimming the overhead lights if possible.
- The proper position has been reached when after advancing the tube, the glow emanates from the midline at the level of the hyoid bone.
- At this point, the stylet is held steady while the tube is carefully advanced off the stylet and into the trachea.
- If the glow is seen somewhere other than the midline at the level of the hyoid bone, withdraw the unit 2 cm or reposition as indicated by the light.
- If no light is seen, esophageal intubation has occurred and the tube should be withdrawn, laryngeal pressure applied, and the head extended slightly; retry placement at this time. (Ensure ambient lighting has been dimmed to optimize viewing)
-
Once the tube is placed, inflate the pilot balloon to the manufacturer-suggested amount of air.
-
Confirm correct placement, secure the tube, and then confirm it again. Monitor continued correct placement en route.
Fiber Optic Intubation
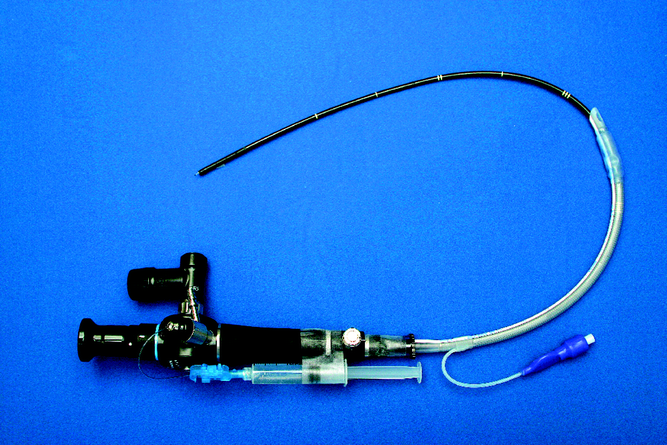
Fiber optic intubation is another type of direct visualized laryngoscopy that uses the same materials and procedural techniques, only with the addition of a small camera at the tip of the laryngoscope blade and a small screen allowing for visualization of the tube passing through the vocal cords. More recently the screen is attached to the handle of the laryngoscope.
If you have difficulty visualizing during direct laryngoscopy, fiberoptic intubation is an excellent way to assist in visualizing your target. It is also very useful when displacing the mandible and tongue prove extremely difficult.
The indications, contraindications, and complications are all largely identical to the use of a lighted stylet. The camera is limited by the tendency of the camera to get covered by secretions.
The Procedure of using the fiber-optic camera is identical to that of a lighted stylet the camera replaces the stylet normally present in the ET tube during intubation. While assembling your equipment be sure to connect and test the camera. Also, have sterile saline on hand to rinse the camera lens if necessary.
Post-intubation reassessment and management
Immediately following intubation carefully monitor every vital sign as countless complications are possible; heart rate, blood pressure, SPO2, ETCO2, and respiratory rate are all critical.
Following the immediate post-intubation period, use the mnemonic DOPE for factors that could affect your now intubated patient while they are in transit.
- D – Displacement/Dislodged tube.
- O – Obstruction or clamped tube.
- P – Placement in the R mainstem bronchus or esophagus.
- E –Equipment: the tube or other equipment may have malfunctioned requiring replacement.