Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
GI Bleeding
Category: Medical
Topic: Abdominal and Gastrointestinal Disorders
Level: EMT
Next Unit: Inflammatory Bowel Disease
17 minute read
DEFINITIONS
Hematemesis: vomiting blood. If fresh, it can be bright red; if older (has remained in the stomach for some time before vomiting, it can assume an appearance of coffee grounds.
Hematochezia: the passage of fresh blood from the anus, usually bright red, indicating recent or current lower GI bleeding.
Melena: the passage of dark, black, or tarry stools from the anus, indicating old blood or bleeding from higher up the intestinal tract.
GI Bleeding
Blood can exit the intact gastrointestinal tract in only one of two ways:
1.) As vomit (upper GI bleeding).
2.) In stool (lower GI bleeding).
Most GI bleeding is an intraluminal event--that is, the bleeding is contained within the lumen of the intact intestinal tract. Rupture of the intestinal walls, as happens with perforation, ulceration, trauma, or infectious erosion, primarily involves danger due to the spillage of bacteria-rich intestinal contents into the sterile abdominal cavity. Therefore, the diagnosis of GI Bleeding is usually confined to bleeding WITHIN the gastrointestinal tract, presenting as blood in vomit, stool, or even both.
Signs of hypoperfusion may be present depending on the amount of blood loss. Patients with a GI bleed can also present with weakness, pallor, and tachycardia. Where possible and tolerable by the patient, take orthostatic vital signs (measuring the blood pressure when supine, sitting, and standing) to see if the blood pressure drops as the patient gets more vertical.
Orthostatic hypotension: the presence of a significant difference when standing indicates that total blood loss is potentially over 1 liter.
Moderate to severe GI bleeds can cause hypovolemic shock, as can any source of bleeding. The body tries to compensate for that lowered volume of blood by increasing the heart rate, and respiratory rate and constricting the peripheral blood vessels, resulting in pallor and clammy skin.
In rectal bleeding, brighter blood is consistent with lower GI bleeds, while dark, tarry stools are more often associated with upper GI bleeds. Old blood is darker--deoxygenated--and the length of the transit time from upper GI to lower GI is enough for the blood to be dark/tarry by the time it makes it to the rectum. Gastric ulcers are sores within the stomach and can produce bright red blood if the patient is vomiting and dark, tarry stools as the blood travels from the area of bleeding to the rectum.
Upper GI Bleeding
Vomiting blood is called hematemesis (hemat = blood) (emesis = vomit.)
- PEPTIC ULCERS
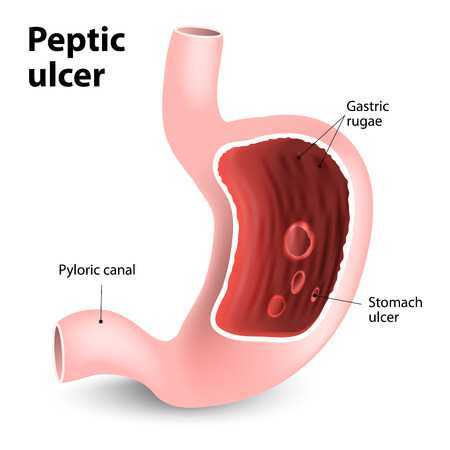
Upper GI bleeds are primarily associated with peptic ulcers but can also be caused by other severe emergencies. Peptic ulcers are caused by an infection of H. pylori bacteria in the GI tract. Ulcers are formed when the protective layer of mucus that lines the GI tract is damaged. Ulcers are prone to present as emergency upper GI bleeding, especially with alcohol abuse.
- MALLORY-WEISS TEAR
A Mallory-Weiss tear occurs when a weakness in the wall of the esophagus or stomach finally ruptures. When this happens, massive bleeding and shock is likely to occur. A Mallory-Weiss tear can also occur with prolonged and/or violent retching, as with hyperemesis of pregnancy. The sheer mechanical stresses of prolonged vomiting can cause a Mallory-Weiss tear.
- ESOPHAGEAL VARICES
Similar in presentation to a Mallory-Weiss tear are esophageal varices, blood vessels near the lower end of the esophagus that become inflamed, dilated, and eventually rupture, causing significant bright red bleeding from the mouth. Alcoholism is the most common cause of esophageal varices due to portal hypertension from liver disease.
Esophageal varices are usually asymptomatic until they burst, resulting in painless hematemesis.
Lower GI Bleeding
Since the GI tract functions to wave contents down its expanse toward the rectum, blood from the upper GI tract will make it down to the lower GI tract, with confusion as to whether the source of blood is upper GI or lower GI.
Frank blood (hematochezia): Usually, if the blood from the rectum is bright red--frank blood--this indicates lower GI bleeding since blood from higher up would have darkened by the time it had reached the rectum.
Occult blood: Slow bleeds are not visible within the stool and are usually only identified by fecal tests. Such blood identified is called occult blood.
Melena: dark blood from the rectum indicates the likelihood of older blood from higher sources.
Causes of lower GI bleeding:
- Diverticulosis: Lower GI bleeds are primarily caused by diverticulosis. Diverticulosis occurs when small sacs (diverticula) develop in the wall of the GI tract.
- Diverticulitis: When the sacs/out pockets of diverticulosis get inflamed or infected, it is called diverticulitis. The most common area for diverticula to form is in the left side of the large intestine, so pain in the left lower quadrant (LLQ) of the abdomen associated with lower GI bleeding can be a tip-off that the cause is diverticulitis.
- Malignancy: The initial presentation of Intestinal cancer may be bleeding--frank and massive or occult/microscopic. Those at risk due to age or family history are screened by their primary care doctors with occult blood stool testing and/or scheduled routine screening colonoscopy, but due to poor patient compliance with what they consider distasteful tests, often go undiagnosed until there is a hemorrhagic emergency.
- Hemorrhoids: Hemorrhoids are a rupture of inflamed varicose veins around the anus and can also be the cause of bright red lower GI bleeding, usually seen as bright red streaks on the stool.
Management of GI Bleeding
Whether blood loss is upper GI, lower GI, or even a gunshot wound, blood loss challenges the homeostasis of a patient and, when severe enough, will manifest as hemodynamic instability:
- Overt hypotension or orthostatic hypotension.
- Tachycardia.
- Dyspnea.
Therefore, treatment for a GI bleed is primarily keeping vigilant and treating the emergence of shock and maintaining a secure airway en route to the hospital.
ABC (airway, breathing, circulation): an advanced airway may need to be placed in cases where the patient is in danger of aspirating blood.
NPO (nothing by mouth): Keep the patient from taking anything by mouth. Ingestion increases the risk of aspiration as well as may delay necessary surgical interventions upon arrival at the hospital.
Position: place them in a position of comfort.
IV access is indicated as well en route to an appropriate surgical facility.