Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Creation of Heart Sounds
Category: Cardiology
Topic: Cardiovascular Anatomy and Physiology
Level: Paramedic
Next Unit: Heart Failure For the EMT Provider
14 minute read
Introduction
Normal heart sounds are the cardiac valves closing--the homeostatic heart heartbeat are auscultated (heard through a stethoscope) over:
- the right second intercostal space at the upper right sternal border (aortic valve),
- the left second intercostal space at the upper left sternal border (pulmonary valve),
- the left third intercostal space at the left sternal border (Erb’s point),
- the left fourth and fifth intercostal spaces at the lower left sternal border (tricuspid valve), and
- the left fifth intercostal space at the left midclavicular line (mitral valve).
There are two normal heart sounds, labeled S1 and S2, and extra heart sounds labeled S3 and S4. The clichéd "Lub-Dub" of the heartbeat heard through a stethoscope minimizes and understates the complexity of what's actually going on.
Lub (S1)
The Lub-: This is called the "First Heart Sound," and for this reason it is designated S1.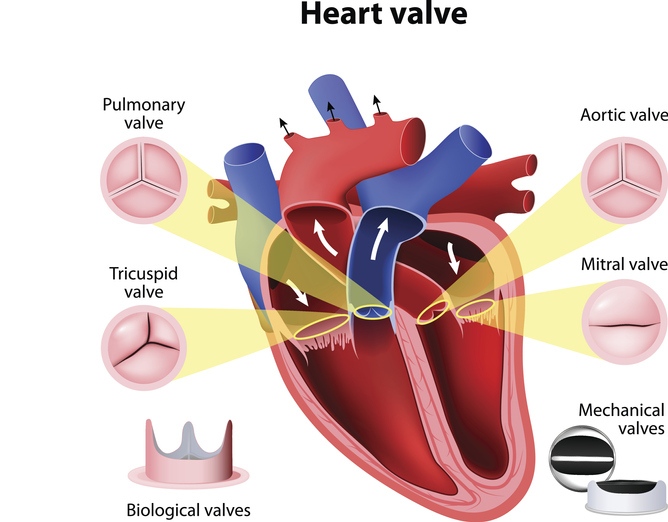
It represents the nearly simultaneous closure of the left and right atrioventricular valves--that is, the mitral and tricuspid valves, respectively, and is created from reverberation within the blood as an effect of the sudden block of blood flow by the valves. Since it occurs first, it represents the beginning of atrial diastole and the initiation of ventricular systole.
S1 is composed of mitral valve closure and tricuspid valve closure, known as M1 and T1, and takes place at the beginning of ventricular contraction (systole).
Normally, M1 occurs slightly before T1, but in certain cases, the order can be reversed, as often found in a left bundle branch block.
Upon ventricular contraction, the pressure from the ventricles contracting cause papillary muscles in each ventricle that are attached to the cusps of the tricuspid and mitral valves via chordae tendineae (heart strings) to become tense and prevent the backflow of blood.
Dub (S2)
The -Dub: This is called the "Second Heart Sound," and for this reason it is designated S2. It represents the closure of the pulmonary and aortic valves, and is created from reverberation within the blood as an effect of the sudden block of flow reversal.
(These two components (P2 and A2) separate a bit on inspiration, but a wide split indicates a conduction-type arrhythmia or hemodynamic causes.)
The S2 sounds--known as A2 and P2--take place at the end of ventricular systole and the beginning of ventricular diastole.
S2 marks the transition from systole to diastole, occurring when aortic (120/80 mmHg) and pulmonary (25/8 mmHg) pressures exceed their ventricular pressures, forcing valve closure. Due to higher systemic pressures, A2 sounds louder and transmits widely, while P2 is best heard at the second left intercostal space.
During inspiration, negative intrathoracic pressure increases right heart filling while decreasing left, creating a normal split S2 (0.02-0.08 seconds). This timing difference between A2 and P2 reflects the temporary delay in right ventricular emptying.
Pathological split S2s help diagnose specific conditions: right bundle branch block (delayed RV depolarization >0.12s), pulmonary stenosis (increased RV afterload), and atrial septal defect (fixed split from constant left-to-right shunt). The split's width and persistence through respiration offer clues to disease severity.
Systole is between the S1 and S2 (between the "lub-" and the "-dub"). Diastole is between S2 and the next S1 (after the "-dub" but before the next "lub-").
Ventricular Filling Sounds (S3 and S4)
S3 and S4 are low-frequency diastolic sounds that originate in the ventricles.
S3
S3 occurs at the beginning of diastole after S2, is lower in pitch than S1 or S2, is not of valvular origin, and is thought to be caused by the oscillation of blood back and forth between the walls of the ventricles initiated by blood rushing in from the atria. As such, it is associated with an enlarged ventricular chamber.
It may also be caused by tensing of the chordae tendineae during rapid filling and expansion of the ventricle. The S3 sound is indicative of an increased volume of blood within the ventricle.
An S3 is able to be distinguished as either left- or right-sided by whether or not it increases in intensity with inhalation or exhalation.
- A right-sided S3 will increase on inhalation, and
- a left-sided S3 will increase on exhalation.
S3 is also known as a protodiastolic gallop.
S4
S4 occurs just after atrial contraction at the end of diastole and immediately before S1, and is caused by the result of blood being forced into a stiff or hypertrophic ventricle. Atrial contraction must be present for S4 to be produced, and the sound is indicative of a pathologic state such as a failing or hypertrophic left ventricle as is found in systemic hypertension, severe valvular aortic stenosis, and hypertrophic cardiomyopathy.
COR PULONALE: Such cardiac repercussion can originate from pulmonary hypertension, called COR PULMONALE (trans., heart disease by way of the lungs). In fact, the 4-toned "Ta-Lub-Dub-Ta" is a sign of cor pulmonale.
Gallops: abnormal S3 and S4 sounds, louder and higher pitched (sharper).
S3 is the ventricular gallop and S4 is the atrial gallop sound.
Murmurs
Murmurs: These are extra sounds heard differently from the S1 and S2 and can be described in relation to both heart sounds. They are the result of turbulence of flow of blood within the heart chambers and are useful in diagnosing valvular diseases that create them. (Turbulence of flow within arteries are called bruits--pronounced "BRU'-eez.")
- Systolic murmurs are heard between S1 and S2 (between the "lub-" and the "-dub").
S1 → SYSTOLIC MURMUR → S2
- Diastolic murmurs are heard between S2 and the next S1 (after the "-dub" but before the next "lub-").
S2 → DIASTOLIC MURMUR → S1