Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Assessment of the Airway, Ventilation, Respiration and Oxygenation
Assessment of Ventilation, Respiration, and Oxygenation (breathing)
Assessment of the airway, ventilation, respiration, and oxygenation begins the second you assume care of a patient. While these assessments make up both the "A" and "B" of the ABC's, they are often grouped together due to their reliance on one another. The section will review the formal elements of the airway and breathing assessment and the basic management of issues regarding these systems.
Assessment of the Airway
The assessment of the airway varies based on the patient's mental status.
The Unresponsive Patient
AIRWAY STATUS: The only absolute indicator of airway status in unresponsive patients is the movement of air. Seeing condensation in oxygen masks, feeling air movement, and using end-tidal CO2 monitors are all good ways of ensuring ventilation is occurring.
DANGER SIGNS: Snoring, gurgling, choking, and coughing are all potential indicators of compromised airways in unconscious patients. If these are occurring, it would be wise to reposition the patient or consider airway-related interventions.
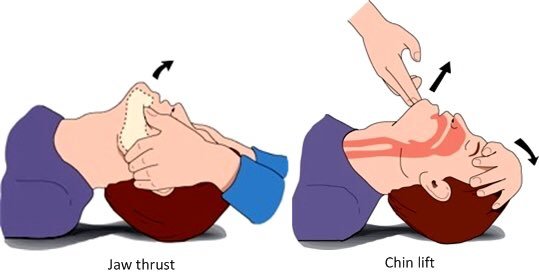
You should open the airway of an unresponsive patient manually. Non-traumatic mechanisms of injury should be managed with the head-tilt, chin-lift technique. Patients with traumatic injuries that may compromise the C-spine are limited to the jaw thrust (also known as the modified jaw thrust) technique. This prevents the potential worsening of an unstable spinal injury. If the airway cannot be maintained with a jaw thrust in a spinal trauma patient, it is appropriate to carefully perform the chin-lift maneuver and manually hold C-spine alignment with the head tilted. This is allowed due to the patency of the airway being one of the key aspects of survival.
The Responsive Patient
The best sign of airway patency in responsive patients is the ability to hold a conversation without changes in the voice or feeling of breathlessness. However, a patient's airway may still be at risk even when they are conversational. Foreign bodies within the mouth or trauma to the face and neck may lead to airway compromise in a conversational patient.
Stridor is a common sign of airway narrowing, generally due to partial obstruction by a foreign body, swelling, or trauma. It is defined as a high-pitched whistling sound upon inspiration.
Assessment of Ventilation
Ventilation is the movement of air in and out of the lungs through a patent airway. The majority of observations regarding ventilation focus on the movements of the chest.
SIGNS OF ADEQUATE VENTILATION: In most patients, your assessment of ventilation will be based on observing their respiratory rate (normal 12 to 20) and listening for clear breathing sounds in the left and right chest. Auditory confirmation of breathing sounds is the strongest sign of adequate ventilation. In patients on ventilators or bag-valve-mask, this does not change.
SIGNS OF INADEQUATE VENTILATION: The signs of inadequate ventilation are best broken down into what you can see and what you can hear.
Visual signs: The visual signs specific to inadequate ventilation are the rate of breathing, abnormal chest wall movement, irregular breathing pattern, and abnormal work of breathing.
Bradypnea (a RR below 12): Generally the result of neurological compromise. Since the RR is closely controlled by the hypothalamus, this is generally the sign of a severe condition. Suspect drug overdose, spinal injury, brain injury, or a severe medical condition when encountering a slow RR.
Tachypnea (a RR over 20): Most often the result of physical exertion. Medical illness and airway obstruction are other common causes. Tachypnea can lead to imbalances in the body's acid-base status or exhaustion of the respiratory muscles.
APNEA: An absence of breathing should be treated with a re-assessment of the airway followed by rapid initiation of mechanical ventilation, generally via bag valve mask. Patients who are gasping occasionally should be treated as apneic until proven otherwise.
The chest should move equally and significantly with each breath. Trauma or penetration can lead to obvious open holes in the chest wall, splinting (reduced movement due to pain), or paradoxical movement (a segment of the chest that moves inward on inspiration).
The pattern of breathing should be predictable. A rapidly changing pattern or absence of breathing are key concerns.
"Work of breathing" refers to the difficulty of taking a breath. Patients at rest should have no difficulty carrying on a conversation without stopping to catch their breath. They should not be using the muscles in their neck or ribs to take a breath, and they should not be sweating or bending over to breathe. *This is not specific to ventilation. Patients with poor oxygenation or poor respiration may also have these same signs.
Auditory signs: The auditory signs specific to inadequate ventilation are abnormal sounds in the chest, a silent chest, or unequal sounds in one side of the chest.
Abnormal sounds commonly heard in the chest are stridor, wheezing, and crackles. Stridor is a high-pitched whistling sound on inspiration, usually in the upper center of the chest that results from upper airway obstruction. Wheezing is a similar sound but in the lower lung fields and results from over-constriction of the lower airways in asthmatics. Crackles are just that, a crackling sound in the lower lung fields, resulting from fluid in the alveoli, such as in pneumonia or drowning.
A silent chest implies significantly reduced airflow into the lungs. This may occur in the setting of pneumothorax, asthma, airway obstruction, or other diseases that block the airways and limit lung expansion.
Unequal breath sounds between the left and right chest are concerning for a process that affects a single lung. Pneumothorax, pneumonia, and obstruction are the three most common causes. Pneumothorax is the presence of air inside the chest cavity but outside the lung, this prevents the lung from expanding and creating breath sounds. Pneumonia causes "consolidation" or stronger breath sounds in combination with crackles in a single area of the chest. Obstruction, caused by the aspiration of solids or liquid can alter breath sounds in a single area of the chest by blocking the bronchiole that leads to that area. This is most commonly seen in the right lung as the position of the right main bronchus is more prone to obstruction, given its angle.
SYMPTOMS OF INADEQUATE VENTILATION: The symptoms of inadequate ventilation, regardless of the cause, are the same. The body only knows that it is not getting enough oxygen and sends strong autonomic signals leading to the following:
Shortness of breath: Also known as "air hunger" or "dyspnea," defined as an inability to carry on a conversation or walk without breathing at an uncomfortable rate.
Cough: Usually occurs due to an obstruction at any level of the airway. Coughing from upper airway obstructions is usually more intense and dramatic, while lower airway obstructions cause longer-lasting chronic coughs.
Thrashing and combativeness: As mental status declines, patients can thrash and become combative as if they were drowning. This ironically increases oxygen consumption and tends to be a sign of impending unconsciousness.
RESPIRATORY PATTERNS
PATTERNS OF BREATHING
Regular pattern:
- Normal breathing.
/¯\__/¯\__/¯\__/¯\__/¯\__/¯\__ - Kussmaul breathing: primarily deep, labored, and often rapid or consistently increased in rate, in response to metabolic acidosis. Deep inspirations attempt to blow off CO2 to raise pH. (E.g., DKA.)
__|¯¯¯¯|__|¯¯¯¯|__|¯¯¯¯|__|¯¯¯¯|__|¯¯¯¯|__
Irregular pattern:
- Cheyne-Stokes: "Periodic Breathing." Periods of increasing depth and rate alternating with periods of decreased rate and shallowness, separated by apnea. ("Crescendo-decrescendo" or "waxing and waning.") In Cheyne-Stokes breathing, the clusters themselves are composed of varying rates and depths, rising and then falling. (E.g., CHF, TBI.)
_|¯|_|¯|_|¯|_|¯|_|¯|________|¯|_|¯|_|¯|_|¯|_|¯|________|¯|_|¯|_|¯|_|¯|_|¯|______
- Biot's respirations: Clusters of similar breaths with irregular timing and unpredictable apneas—not a regular rhythm of clusters. This pattern distinguishes Biot's respirations from Cheyne-Stokes (which is regular and cyclical) and ataxic breathing (which is even more disorganized and irregular in depth and timing).
_|¯|__|¯|_|¯|______|¯|_|¯|___|¯|__|¯|______|¯|__|¯|_|¯|__|¯|___________|¯|___|¯|_|¯|___
Assessment of Respiration
Respiration is the process of alveolar gas exchange, where oxygen enters the blood and carbon dioxide is removed. Since it cannot be directly observed, assessment is difficult, and conditions involving ventilation, oxygenation, or gas exchange often overlap, adding to the challenge.
Assessing respiration generally requires information about the environment the patient was found. The presence of poor air quality is a sign of potential respiration-related issues. Enclosed spaces, extremely high altitudes, and known exposure to toxic gases can all dramatically affect the respiratory system.
Loss of respiratory capacity can lead to changes in the color of the skin and mucosa: cyanosis (blue discoloration), pallor (white discoloration), and mottling (patchy red-purple) discoloration are common findings that suggest gas exchange has been compromised.
Assessment of Oxygenation
Oxygenation is the delivery of oxygen to the tissues of the body. Poor ventilation or respiration will generally lead to poor oxygenation. Loss of oxygenation is the ultimate result of ventilatory or respiratory failure.
Assessment of oxygenation is more direct than assessing respiration or ventilation. You need to observe the patient's mental status, skin color, oral mucosa, and check a pulse oximeter.
Mental status is either normal or abnormal. Assessing mental status is based on asking questions about who the person is, what time/date it is, where they are, and why they are here. Mental status is reviewed in other sections.
Skin and mucosal color are important indicators of oxygenation. Just as with poor respiration, cyanosis, pallor, or mottling are signs of decreased oxygen delivery.
Finally, the pulse oximetry level is the most objective measure of oxygenation, it reads the saturation of hemoglobin (reported as SPO2). Note that a pulse oximeter is not foolproof. A patient with poor oxygenation in the limbs may have sufficient oxygenation to their core or vice versa. Pulse oximeters can also be fooled by specific toxic gases. Always ensure that you match up your pulse oximetry readings with physical findings and ensure they support one another.
PULSE OXIMETRY: Pulse oximetry should be used as a routine vital sign but is contraindicated and known to be unreliable in certain situations. The most common of these situations are; Hypoperfusion, carbon monoxide poisoning, and hypothermia are all conditions that can reduce the accuracy of a pulse oximeter.
Pulse oximeters are imperfect and are not a real-time measure of O2 saturation. The blood needs to transit from the heart and lungs to the fingertips prior to obtaining a reading. For example, a patient in relatively good health could have stopped breathing for some time, and the SPO2 reading may stay relatively high for a while; don’t rely only on the snapshot of an SPO2 as a reliable assessment of oxygenation. Treat the patient, not the monitor.
Refer to the manufacturer’s instructions for the specific device being used. Always consider alternative measurement sites.
Additional Important Concepts
SPECIAL POPULATIONS: Pediatric patients and geriatric patients have different demands for oxygen when compared to average middle-aged adults, thus, physical differences in normal values of respiration rate, depth, and quality are evident.
- Newborns (birth to 1mo) respire at 30 to 60 BPM
- Children (1mo to 12y) respire at 20 to 30 BPM
- Elderly patients who are healthy respire at 12 to 18 BPM, those in poor health 16 to 25 BPM
- Elderly individuals always have an increased need for oxygen, but those with medical conditions are elevated even more so.
PREGNANCY: Pregnancy makes breathing more difficult. The increased upward pressure from the growing fetus restricts the downward movement of the diaphragm. Naturally, the difficulty of breathing increases the further along the woman is in pregnancy. In the third trimester, many women make increased use of the accessory muscles, which can cause costochondritis.
Recumbent (lying or reclining) positions worsen pregnancy-related breathing difficulty. Dyspnea due to pregnancy can likewise be relieved by sitting the patient up or elevating the head-of-bed to a 45° or greater angle.
Patients with twins or triplets may require supplemental oxygen due to the significant growth of the uterus. This can occur as early as the second trimester.
MINUTE VENTILATION: The amount of air that a person breathes per minute is found by multiplying the respiratory rate (RR) by the tidal volume (Vt). (RR x Vt = Minute Ventilation).
Example: RR: 12/min X Tidal Volume of 500ml = Minute Ventilation of 6,000ml/min or 6L/min.