Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
ACLS Tachycardia
Category: Cardiology
Topic: Advanced Cardiac Life Support
Level: Paramedic
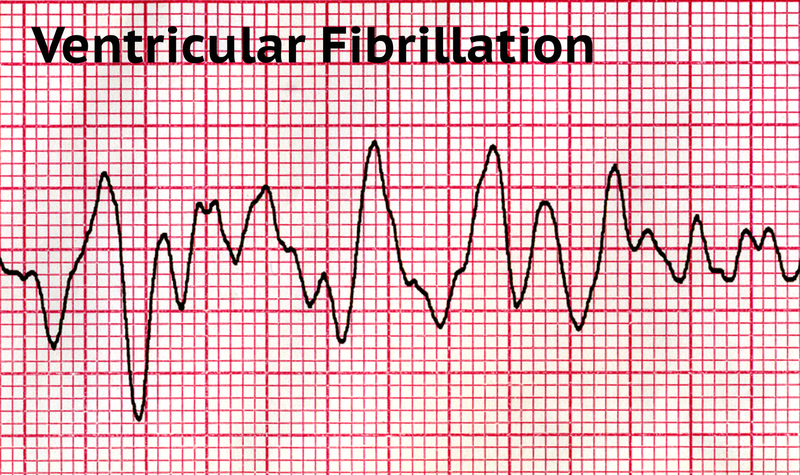
Next Unit: Pulseless Arrest - Ventricular Fibrillation/ Ventricular Tachycardia
19 minute read
Identifying tachycardias isn't exactly rocket science, but it can be intimidating. Don't let the speed of it throw you off! Knowing what to look for and understanding the treatment will allow you to properly identify life-threatening tachycardias and prepare you to make the right clinical decision for the patient.
Let's look at the need-to-know criteria:
RATE:
- Normal resting adult heart rate is typically between 60-90 bpm.
- Normal active (aerobic activity) heart rate is typically between 110-180 bpm during the activity and for a brief time immediately after during the "cool down" stage.
QRS:
- A wide QRS complex is anything > 0.12 seconds (120 milliseconds) or 3 small boxes.
- A Narrow QRS complex is < 0.12 seconds (120 milliseconds).
REGULARITY:
- Is the cardiac rhythm regular? Think: "normal sinus regularity."
- Is the cardiac rhythm irregular? Think: "atrial fibrillation irregularity."
SYMPTOMATIC vs ASYMPTOMATIC:
- Is the patient pale, cool and clammy with altered mentation and an HR of 170?
- Are they sitting calmly in their doctor's office, asymptomatic, with an HR of 150?
LIFE-THREATENING vs STABLE:
- Must something be done immediately (IV/IO, cardioversion, CPR) or do you perform your typical tasks (IV, cardiac monitoring, 12-lead, ASA) and monitor for changes?
- Is this patient without peripheral pulses and unresponsive at a rate of 210?
- Is patient weak, A+Ox4, normotensive and a GCS of 15 at an HR of 160?
Noteworthy Tachycardias
- NARROW-COMPLEX TACHYCARDIAS: QRS < 120 milliseconds
- Supraventricular Tachycardia (SVT): A dysrhythmia originating at or above the atrioventricular (AV) node and is defined by a narrow complex (QRS < 120 milliseconds) at a rate > 150 beats per minute (bpm).
- Supraventricular Tachycardia (SVT): A dysrhythmia originating at or above the atrioventricular (AV) node and is defined by a narrow complex (QRS < 120 milliseconds) at a rate > 150 beats per minute (bpm).
- WIDE-COMPLEX TACHYCARDIAS: QRS > 0.12 seconds:
- Ventricular Tachycardia (VT),
- Ventricular Fibrillation (VF),
- Ventricular paced rhythms
- IRREGULAR TACHYCARDIAS:
- A-fib,
- A-flutter,
- Polymorphic VT.
Medications
MEDICATIONS (per the "ACLS Tachycardia in Adults" algorithm):
- ADENOSINE: 1st dose 6mg--RAPID IVP; 2nd dose 12mg--RAPID IVP.
Adenosine "resets" electrical activity in the heart and attempts to resolve re-entry by blocking electricity traveling through the AV node. You may notice a period of bradycardia (or even asystole) after giving this to your patient that should resolve within 5-30 seconds. Prepare your patient for this before giving Adenosine--a really good idea.
- Antiarrhythmic Infusions for STABLE Wide-Complex Tachycardias:
- PROCAINAMIDE: 20-50mg/min with MAX dose at 17mg/kg/min.
- AMIODARONE: 150mg over 10min, repeat if VT recurs, then 1mg/min for 6hrs.
- SOTALOL: 100mg over 5 minutes (1.5mg/kg). ►Avoid with prolonged QT.
H's and T's
IDENTIFY AND TREAT UNDERLYING CAUSES (H's & T's).
- If this is a trauma patient who has uncontrolled bleeding from the leg with a heart rate of 155, STOP THE BLEEDING!
- If they have a fever of 103.9° and have wet lung sounds and a heart rate of 140, sepsis would be the major concern here and care should be directed as such.
Signs & Symptoms of PERSISTENT TACHYCARDIA
Persistent tachycardia will affect the rest of the body. Symptoms that may present are:
- Hypotension.
- Altered mental status.
- Signs of shock.
- Increased weakness and lethargy.
- Chest pain.
- Hypoxia.
To Shock or Not to Shock: That is the Question
If a patient is symptomatic as listed above and no other causes are found (such as trauma or possible infection), chemical and/or electrical cardioversion is the next step.
According to the ACLS algorithm for tachycardia in adults,
- an unstable patient requires synchronized cardioversion with sedation as possible.
Do not delay cardioversion if the patient is extremely unstable.
- For patients who have regular narrow-complex tachycardia such as SVT, adenosine is indicated.
TO SHOCK: -
- 50 y.o.m. with regular narrow-complex at 200 bpm who is pale and altered--with no suspected trauma--and has a pulse but is not responsive to adenosine.
- 63 y.o.f. with regular wide-complex at 160bpm who is hypotensive with MAP <50 with no suspected trauma and has a pulse.
NOT TO SHOCK:
- 90 y.o.f who is responsive and at her baseline in appearance and mentation, with regular narrow-complex at 140 bpm who can vagal down and slow-rate to 100.
- 47 y.o.m with irregular wide-complex at 130-200 who has a MAP of 50.
Consider procainamide at 20-50mg/min. Consult medical direction as needed. ►DO NOT USE PROCAINAMIDE AT THE SAME TIME AS AMIODARONE WHICH CAN CAUSE PROLONGED QT INTERVALS.
PULSE vs NO PULSE:
ALWAYS check a peripheral pulse. If they are unresponsive, check centrally (carotid/femoral).
►If no pulse, START CPR!
Symptomatic vs Asymptomatic
- What does the patient look like?
- Are they pale, cool and diaphoretic?
- Are they tachypneic?
- Are they altered? or do they appear like nothing is wrong and they aren't sure why you have that concerned look on your face?
As with anything else in evaluating our patients, changes in skin condition, respirations, and mental status can be key indicators of something amiss.
For example, Mr. Smith, who is 73 years old and looks like he just completed the Boston Marathon with a sustained heart rate of 180 needs immediate attention and more than likely cardiac intervention.
- Monitor for reversible causes with H's and T's and treat as necessary.
Vagal Maneuvers
"Puttin' on the brakes": The right vagus is a parasympathetic inhibitor of SA node stimulation; the left vagus is a parasympathetic inhibitor at the AV node. With SVT, the effect of vagal maneuvers will predominate in the SA node, making it a first--and safe--method of decreasing the heart rate in supraventricular tachycardia. It works in 7 out of 10 SVTs.
Vagal maneuvers are parasympathetic stimulations that release acetylcholine that:
- SA node impulses slow down.
- AV node conduction slows down (refractory period gets longer).
TYPES OF MANEUVERS:
- Valsalva--possibly works best with SVT, so start with it. It consists of attempted (blocked) force expiration against a closed nose and mouth.
- "Modified" Valsalva Maneuver--do the Valsalva, then lay the patient supine with a 45°-angle leg raise for 15 seconds.
- Carotid sinus massage--useful when there is carotid sinus hypersensitivity--with the patient supine, apply constant pressure (some do vigorous circular motions) to one carotid sinus for 5-10 seconds; if no response do the other side. (If the expected response is not obtained, the procedure is repeated on the other side after a one- to two-minute delay.)
- Diving Reflex--cumbersome, so not high on the to-do list for SVT.
With your patient seated in front of a tub of cold water, while attached to telemetry, he/she takes a deep breath, holds it, then places his/her face into the tub of water for about a half-minute, if possible, for 20 to 30 seconds. Both the facial exposure to cold (cold exposure to the ophthalmic division of the trigeminal nerve--important for the response) and the breath-holding cause both a parasympathetic bradycardia and a sympathetic peripheral vasoconstriction, ending the SVT.
- Oculocardiac Reflex--pressing on the eyeball(s) stimulates the vagus nerve (via stimulation of the ophthalmic branch of the trigeminal never. Normally, this vagal maneuver is not used.
The Poor Man's Adenosine: the heart rate and rhythm after any vagal maneuver is similar to the administration of adenosine:
- SA node slowing.
- Inhibiting the AV node, which will make the atrial activity more observable.
- Ending SV.
- Of course, one possible response is no response. (Keep the adenosine ready--6 mg rapid IV bolus over 1-2s; after 1-2 minutes, 12-mg dose over 1-2 seconds; IV with 20cc flush.)